
Primary Health Care Operating System (PHC-OS)
The gap is operational, not informational
PHC-OS is a proposed computational architecture for comprehensive primary health care delivery at scale. Optimize Health is working to build it and to support its development across the field.
Why this is needed
Coordinating comprehensive primary health care for a defined population means orchestrating thousands of asynchronous actions across homes, clinics, and providers, over time, for every individual. For a catchment of 5,000 people, even a modest set of indicated actions per person per year produces tens of thousands of coordination decisions.
No manual system can manage this combinatorial complexity reliably. No point-solution — however sophisticated — addresses it. What the field calls a delivery gap is, more precisely, an integration gap: the absence of an architecture that encodes care pathways, integrates the tools that support each step, and orchestrates delivery across a whole population.
What it would be
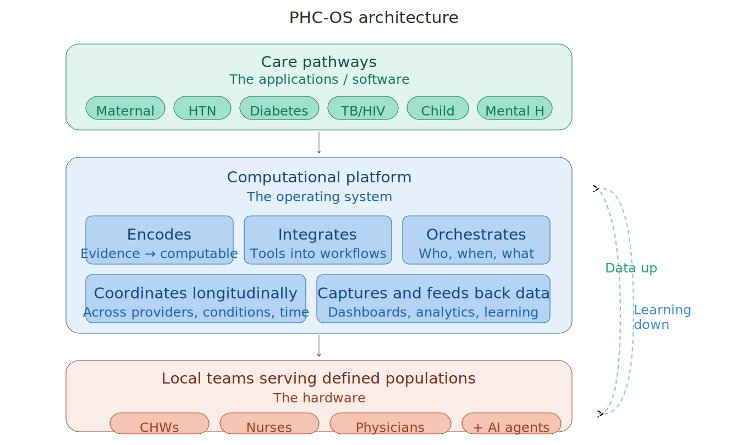
A primary health care operating system, as we conceive it, would be a computational platform that coordinates the delivery of comprehensive primary care for a defined population — analogous to how a computer operating system coordinates applications, hardware, and data.
It would do three things. It would encode what should be done for each health condition into computable care pathways, drawing on guidelines, evidence, and clinical consensus. It would integrate the digital and AI tools that support each step of care into the workflows of frontline teams. And it would orchestrate delivery across providers and over time, ensuring that the right care happens for the right person at the right moment, and that what gets done feeds back into how the system learns.
This is not an AI system. It is a delivery architecture into which AI, digital tools, and innovations in care could continuously integrate. The architecture stays constant; capabilities at each node advance.
What it looks like in practice
Consider a typical case. A 52-year-old man in a rural village is found to have elevated blood pressure during a community health worker's home visit. The system triggers a hypertension pathway: confirmatory readings are scheduled, medication is initiated by protocol, monitoring visits are queued. Comorbidity logic flags him simultaneously for diabetes screening. When fasting glucose returns elevated, a second pathway activates alongside the first.
The system coordinates both. Visits are consolidated. Medications are checked against each other. Monitoring frequency adjusts for the dual diagnosis. When titration exceeds nurse-level protocols, he is routed to a physician through telemedicine, with the full longitudinal record at the point of consultation. If a refill is missed, a community health worker is alerted. If renal function declines, a referral fires with the relevant context attached.
No single tool does this today. Each component step — screening, scheduling, prompting, routing, escalation — is amenable to rule-based coordination. What does not yet exist is the architecture that connects them across conditions, providers, and time, for one patient and across the population a team serves.
From vertical pathways to integrated delivery
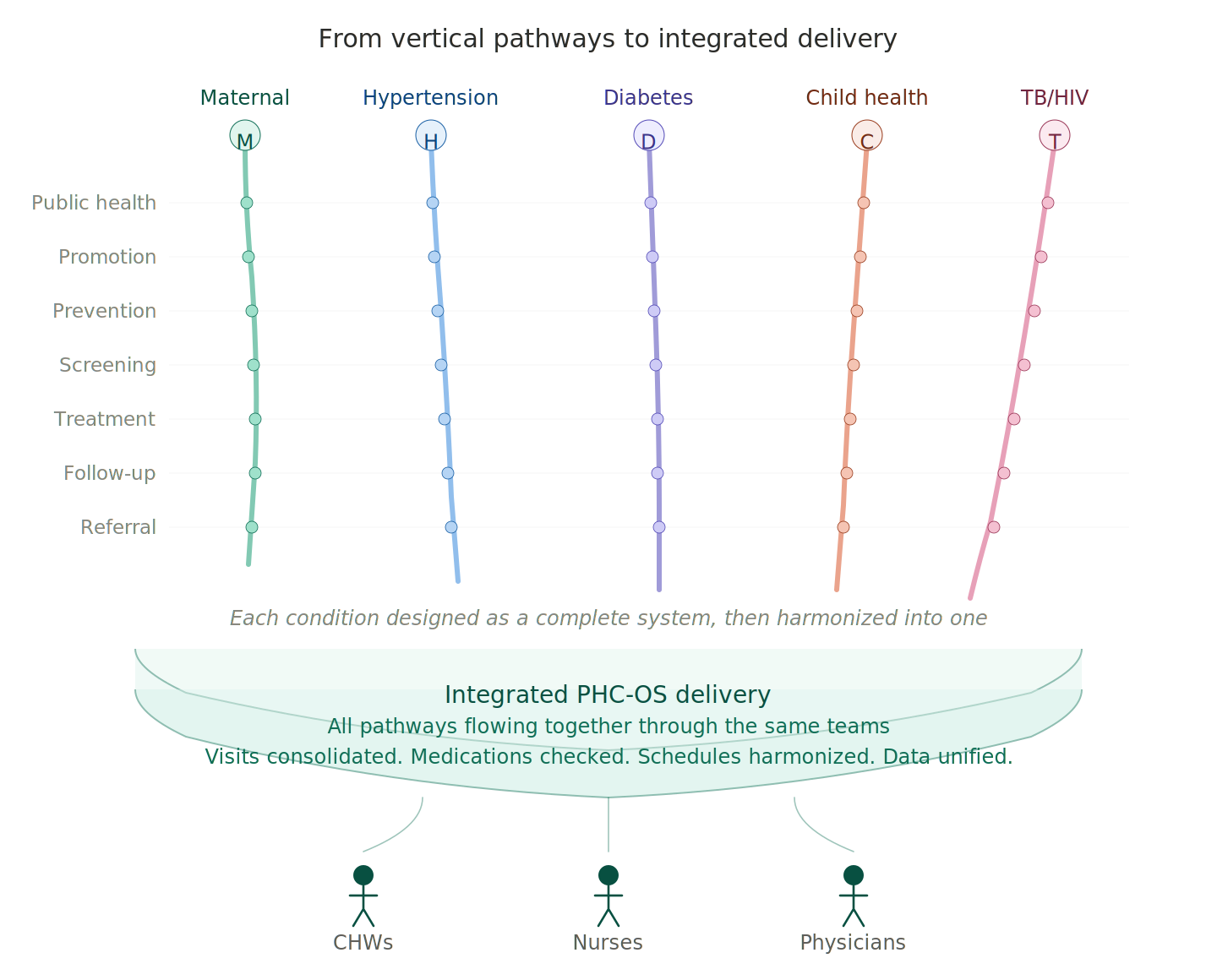
PHC-OS is conceived around a specific architectural principle. Each condition's care pathway would be designed as if the entire system existed for that condition alone — fully specified across screening, treatment, monitoring, follow-up, and referral, with the depth that vertical disease programs have historically achieved. All pathways would then be harmonized into a single horizontal delivery system, prioritized by policy and local epidemiology, delivered through the same teams.
The vertical depth would be preserved in the encoding. The horizontal integration would be achieved in the delivery. A community health worker visiting a household would not run a maternal program one day and a hypertension program another. The same worker, the same visit, the same data system would manage whatever care each member of the household needs.
Buildable today, progressively more powerful
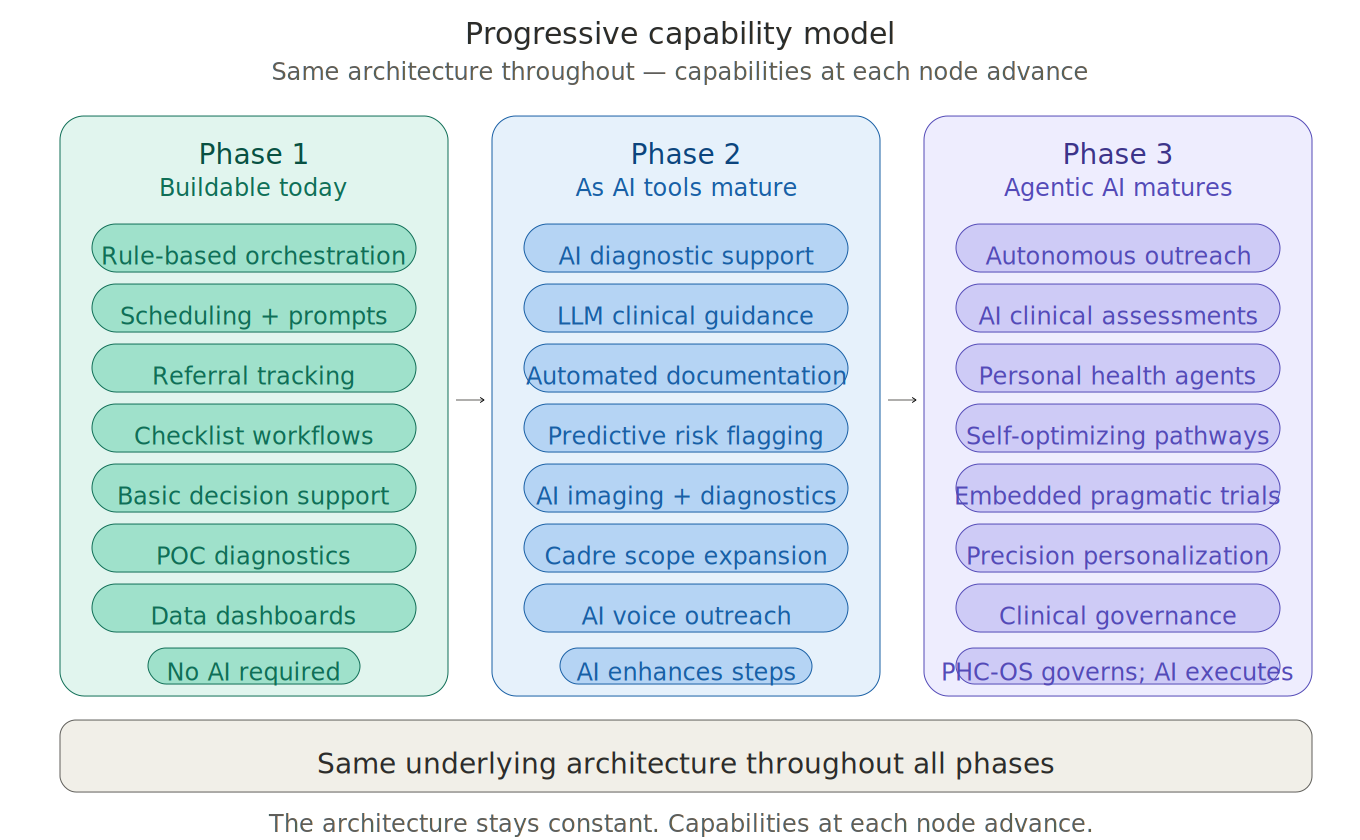
PHC-OS could be built today, with no artificial intelligence required. Most of what falls through the cracks in primary care is not a failure of clinical judgment but of operational coordination — scheduling, tracking, prompting, referral routing, escalation. These are problems amenable to rule-based logic, and the digital infrastructure to support them already exists.
The architecture is designed to absorb more capable tools as they mature: AI diagnostic support and clinical guidance as those tools are validated, then increasingly autonomous capabilities — automated documentation, AI-mediated outreach, agentic care coordination — as the technology advances. The architecture stays constant. Capabilities at each node advance.
In concert with the field
PHC-OS is intended to operate alongside the work others are doing in primary health care, not in competition with it. Across India and globally, organizations have developed strong approaches to specific elements of care — community health worker programs, diagnostic protocols, chronic disease management, telemedicine workflows, supply chain logistics, patient engagement.
What is often missing is not more individual innovations; it is the integration layer that lets them function together as comprehensive primary care for a defined population. PHC-OS is meant to be that layer — open, interoperable, able to incorporate proven components and orchestrate them as a coherent system rather than as parallel tracks. The aspiration is consolidating ground for the field's best work, not a parallel track to it.
Public-good infrastructure
A primary health care operating system should not be a proprietary product. Like the public health infrastructure it operates within — clinics, registries, surveillance systems, immunization programs — it should be developed as a social good, governed by public or government entities, and accessible to the populations it serves.
This is a deliberate position. PHC-OS is meant to be the substrate on which the field's best work can be assembled, propagated, and improved. That substrate is most useful when it is open, interoperable, and free of the constraints that come with private ownership of critical infrastructure. National digital health architectures, regulatory standards for clinical care, and the data generated by population-level care all sit naturally in the public sphere. A PHC-OS should sit there with them.
In practice, this means the technical architecture should be open and aligned with national digital health standards. The care pathways encoded into the system should reflect the clinical consensus of the public health community rather than the priorities of any single organization. The data the system generates should serve the populations it's drawn from — for surveillance, for equity monitoring, for continuous improvement — not be captured as a commercial asset. Governance should ultimately rest with public entities accountable to the people the system serves.
Optimize Health's role is to demonstrate the framework, develop the components, and contribute to the field — not to own the platform. Our work is supported by philanthropic funding. We do not sell, license, or commercialize software or technology. The PHC-OS we are working to build is intended as public-good infrastructure from the outset.
Reference
The full PHC-OS framework is detailed in:
The Primary Health Care Operating System: A Framework for Encoding and Orchestrating Comprehensive Care Delivery — preprint available on SSRN.
For correspondence about the framework or about Optimize Health's work: info@optimize.org